When your blood calcium stays too high for too long, your body starts breaking down. Not from overdoing it at the gym or eating too much dairy-this is something deeper. It’s called hyperparathyroidism, and it’s not rare. Around 100,000 people in the U.S. are diagnosed each year, mostly women over 50. Most don’t feel sick at first. But over time, the damage adds up: bones weaken, kidneys form stones, and your brain feels foggy-not from stress, but from calcium levels that won’t quit.
What’s Really Going On in Your Body?
Your parathyroid glands are four tiny pea-sized organs behind your thyroid. They don’t make thyroid hormone-they control calcium. Every time your blood calcium dips, they release PTH (parathyroid hormone) to pull calcium from your bones, boost absorption in your gut, and tell your kidneys to hold onto it. Simple. Smart. Until it goes wrong. In primary hyperparathyroidism, one or more of these glands start producing too much PTH on their own. Usually, it’s a benign tumor-called an adenoma-growing silently on one gland. In 15% of cases, all four glands are enlarged. Less than 1% are cancerous. The result? Calcium levels climb above 10.5 mg/dL. Normal is 8.5 to 10.2. When it hits 12 or higher, you’re in danger zone. This isn’t just a lab number. Excess PTH turns your bones into calcium factories. Your osteoclasts-cells that break down bone-go into overdrive. Studies show people with untreated hyperparathyroidism lose 2-4% of bone density every year at the hip and spine. That’s not normal aging. That’s accelerated osteoporosis. By the time someone hits 60 with this condition, their fracture risk is 30-50% higher than peers with normal calcium.Why You Might Not Realize You Have It
Many people with hyperparathyroidism have no obvious symptoms. That’s why it’s often found by accident-during a routine blood test for something else. But when symptoms do show up, they’re easy to misread:- Chronic fatigue that doesn’t improve with sleep
- Joint or bone pain, especially in the back or hips
- Kidney stones-repeatedly, even if you drink plenty of water
- Brain fog, trouble concentrating, or memory lapses
- Depression or anxiety that doesn’t respond to therapy
How Doctors Diagnose It
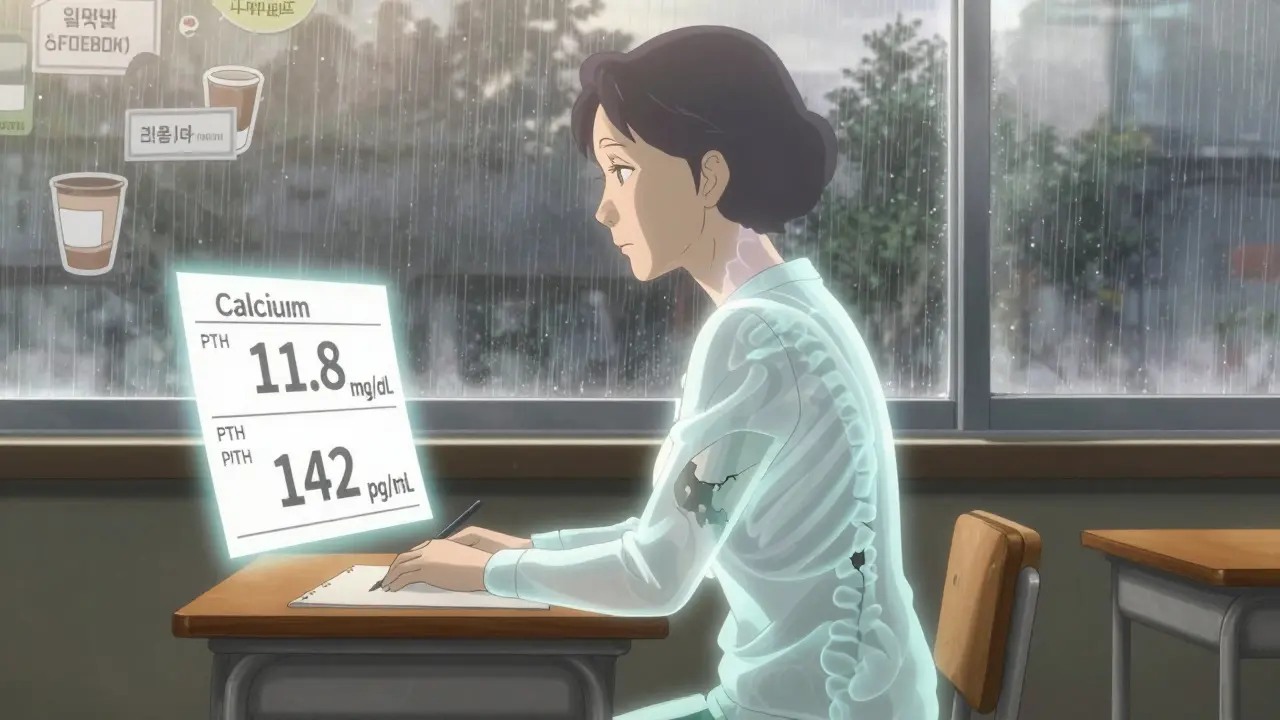
Diagnosis starts with two simple blood tests: serum calcium and parathyroid hormone. But here’s the catch: if your calcium is high and your PTH is normal or even “in range,” that’s still abnormal. Healthy glands would shut off PTH when calcium is up. If it’s still high, your glands aren’t listening. That’s hyperparathyroidism. Doctors confirm it by repeating the test a week later. One high result could be a fluke. Two? That’s a pattern. Next comes imaging to find the culprit:- Technetium-99m sestamibi scan: 90% accurate at spotting a single adenoma. It lights up the overactive gland.
- High-resolution ultrasound: Checks for swelling or nodules in the neck. 85% accurate.
- 4D-CT scan: Used for complex cases. 95% accurate, especially if previous scans were unclear.
Surgery: The Only Cure
Medication can manage symptoms, but it doesn’t fix the root problem. Cinacalcet lowers PTH a bit, and bisphosphonates slow bone loss-but neither stops the gland from overproducing. Only surgery does. The procedure, called a parathyroidectomy, removes the bad gland(s). For the 85% of patients with a single adenoma, it’s a minimally invasive outpatient surgery. A tiny incision, 1-2 hours, and most people go home the same day. Recovery? Usually 3-7 days. Success rate? 95-98% when done by experienced surgeons. For those with multiple enlarged glands, surgeons remove 3.5 glands (leaving a sliver behind to prevent lifelong low calcium). Success drops slightly to 85-90%, but it still works. Post-op, calcium levels can dip too low temporarily-this is normal. About 30-40% of patients need calcium and vitamin D supplements for a few weeks. A few may need them longer, especially if they had severe bone loss.Who Needs Surgery-and Who Doesn’t
Not everyone with high calcium needs surgery right away. But guidelines from the Endocrine Society say you should consider it if you meet any of these:- Calcium is more than 1 mg/dL above normal
- Your kidney function is low (creatinine clearance under 60 mL/min)
- Your bone density T-score is -2.5 or worse
- You’re under 50 years old
- You’ve had kidney stones
What Happens After Surgery?
Most people see big improvements within months:- 88% report less bone and joint pain
- 92% have fewer kidney stones
- 75% say their energy and focus return
What to Do Now
If you’ve been told your calcium is high, don’t wait. Ask for a PTH test. If it’s elevated, ask for imaging. If you’re over 50, especially a woman, and you’ve had unexplained fatigue, bone pain, or kidney stones-get checked. Many doctors still miss this. If surgery is recommended, find a surgeon who does at least 50 parathyroidectomies a year. Volume matters. High-volume centers have 98% success rates. Low-volume ones? Closer to 85%. And if you’re scared of voice changes? Understand this: the risk of permanent vocal cord damage is less than 1% with experienced surgeons. Most people’s voices return to normal in days. This isn’t a condition you live with. It’s one you fix. And fixing it doesn’t just prevent fractures or kidney stones-it brings back your life.Can hyperparathyroidism be cured without surgery?
No. Medications like cinacalcet or bisphosphonates can help manage symptoms or slow bone loss, but they don’t remove the overactive gland. Only surgery can cure primary hyperparathyroidism by removing the source of excess PTH. Without surgery, calcium levels stay high, and bone and kidney damage continue to progress.
How long does it take to recover from parathyroid surgery?
Most people go home the same day. Pain is usually mild and lasts 1-3 days. Full recovery-returning to normal energy levels, work, and activity-takes 3 to 7 days for most. Bone pain and fatigue may take weeks to months to fully improve, especially if bone loss was severe. Calcium levels are monitored closely for the first 72 hours after surgery.
Is hyperparathyroidism hereditary?
About 10% of cases are linked to inherited syndromes like MEN1 (multiple endocrine neoplasia type 1) or familial isolated hyperparathyroidism. If you’re diagnosed under 40 or have a family history of endocrine tumors, genetic testing is recommended. Most cases, however, are sporadic and not passed down.
Can low vitamin D cause hyperparathyroidism?
Low vitamin D doesn’t cause primary hyperparathyroidism, but it can make it worse. When vitamin D is low, your body makes more PTH to compensate-this can mask the true PTH level from the overactive gland. Doctors always check and correct vitamin D levels before surgery, because low levels can lead to severe post-op low calcium.
What happens if I don’t have surgery?
Without surgery, calcium stays high. Over time, this leads to progressive bone loss, increased fracture risk, kidney stones, and possibly kidney damage. Fatigue, brain fog, and depression often worsen. Studies show people with untreated hyperparathyroidism have a 2-3 times higher risk of fractures and higher hospitalization rates. While some choose monitoring, the damage is cumulative and often irreversible after years.















Rajni Jain
December 25, 2025 AT 23:41