Pancreatic Duct Blockage Education Planner
Your Personalized Education Plan
This plan is designed to help you better understand your condition and participate actively in your care.
Living with a blocked pancreatic duct can feel like a never‑ending puzzle. The pain, digestive issues, and anxiety about future procedures are real, but the missing piece that often turns the tide is clear, consistent patient education. When patients understand what’s happening inside their body and how daily choices affect outcomes, they become active partners in care rather than passive bystanders.
Quick Takeaways
- Understanding the cause of blockage helps patients recognize early warning signs.
- Targeted education on diet, medication, and procedure prep reduces hospital readmissions.
- Multi‑format tools (videos, apps, brochures) improve retention for diverse learning styles.
- Regular checkpoints let clinicians measure knowledge retention and adjust plans.
- Empowered patients report lower pain scores and better quality of life.
What Is Pancreatic Duct Blockage?
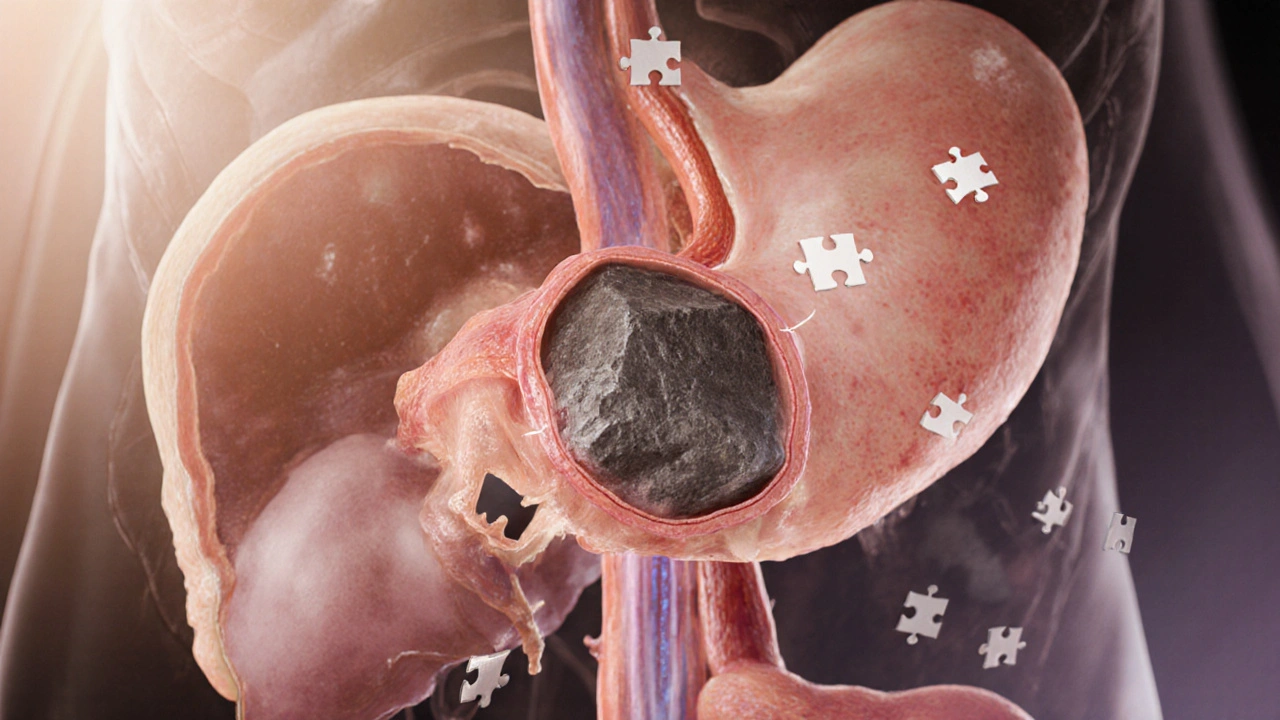
Pancreatic duct blockage is a condition where the main duct that carries digestive enzymes from the pancreas into the duodenum becomes obstructed by stones, strictures, or tumors. The blockage prevents enzymes from reaching the intestines, leading to inflammation, pain, and malabsorption.
Common causes include chronic pancreatitis, gallstone migration, and pancreatic cancer. Symptoms often start with upper‑abdominal pain that radiates to the back, greasy stools, unexplained weight loss, and occasional jaundice. If left untreated, the pressure buildup can trigger severe pancreatitis or infection.
Why Patient Education Makes a Difference
Studies from gastroenterology centers in the UK and US show that patients who receive structured education are 30% less likely to experience emergency visits related to pancreatic complications. Knowledge equips them to:
- Identify red‑flag symptoms early (e.g., sudden fever, worsening pain).
- Adopt dietary habits that reduce enzyme buildup.
- Follow medication schedules for enzyme replacement therapy.
- Prepare effectively for interventions such as Endoscopic Retrograde Cholangiopancreatography (ERCP) or stent placement.
When patients feel confident, they engage more actively during consultations, ask pertinent questions, and adhere to post‑procedure instructions-directly translating into better clinical outcomes.
Core Topics Every Education Session Should Cover
- Understanding the anatomy: Explain the role of the pancreatic duct and why blockage disrupts digestion.
- Recognizing symptoms: List early warning signs and when to call a doctor.
- Medication management: Guide on pancreatic enzyme replacement, dosage timing, and potential side effects.
- Dietary modifications: Emphasize low‑fat meals, adequate hydration, and the importance of spacing meals to lower ductal pressure.
- Procedure preparation: Detail what to expect before, during, and after ERCP or stent placement, including fasting instructions and consent forms.
- Post‑procedure care: Cover pain management strategies, activity restrictions, and signs of stent migration.
- Follow‑up imaging: Explain the role of CT, MRI, or ultrasound in monitoring duct patency.

Choosing the Right Education Tools
| Format | Engagement Level | Cost Approx. | Best For |
|---|---|---|---|
| Printed brochure | Low | £0.50 per copy | Older patients preferring tangible material |
| Animated video | Medium‑High | £150 production | Visual learners, clinic waiting‑room use |
| Interactive mobile app | High | £2,000‑£5,000 development | Tech‑savvy patients needing reminders |
| One‑on‑one counseling | Very High | Staff time (≈£30 per session) | Complex cases, language barriers |
Mixing at least two formats-say, a short video followed by a brief in‑person Q&A-covers a broader audience and reinforces learning.
Building a Patient Education Plan: Step‑by‑Step
- Assess baseline knowledge: Use a quick questionnaire to gauge what the patient already knows about the pancreas and blockage.
- Set clear objectives: For example, “Patient will be able to list three red‑flag symptoms within one week.”
- Select appropriate materials: Choose the format(s) that match the patient’s learning style and health literacy.
- Deliver content: Combine visual aids with verbal explanations; encourage the patient to repeat key points.
- Confirm understanding: Ask the patient to teach back the main concepts. Document any gaps.
- Provide take‑home resources: Hand out a concise checklist covering diet, medication, and when to seek help.
- Schedule follow‑up: Review knowledge retention during the next clinic visit or via a phone call.
Documenting each step in the electronic health record ensures continuity if another clinician takes over.
Common Pitfalls and How to Avoid Them
- Information overload: Too much detail at once overwhelms patients. Break content into bite‑size modules.
- Medical jargon: Replace terms like “exocrine insufficiency” with simple phrases such as “your body isn’t getting enough enzymes.”
- Assuming literacy: Use plain language and visual icons for low‑literacy patients.
- Neglecting cultural factors: Tailor dietary advice to cultural food preferences; consider translation services.
- Skipping reinforcement: One-off sessions fade quickly. Set reminders via text or app notifications.
Measuring the Impact of Education
Track these simple metrics:
- Rate of ERCP‑related complications (aim for <10% reduction).
- Patient‑reported pain scores before and after education (target 2‑point drop on a 0‑10 scale).
- Adherence to enzyme therapy (monitor pharmacy refill data).
- Frequency of emergency department visits for pancreatic pain.
Regularly reviewing these numbers helps refine the education program and demonstrates value to hospital administrators.
When patients walk away from the clinic knowing exactly what to eat, when to take medication, and which symptoms demand immediate attention, they become partners in preventing future blockages. That partnership-fueled by clear, compassionate education-is the cornerstone of long‑term management.
pancreatic duct blockage can be better controlled when patients understand their condition and take an active role in care.
Frequently Asked Questions
What causes a pancreatic duct blockage?
The most common causes are chronic pancreatitis, gallstones that migrate into the duct, and tumors that compress or invade the duct wall. Less frequent reasons include scar tissue after surgery and congenital narrowing.
Can diet alone unblock the duct?
Diet alone rarely clears an obstruction, but a low‑fat, high‑fluid diet reduces pressure on the duct and can prevent worsening. In many cases, medical or endoscopic interventions are needed.
What should I do if I experience sudden severe abdominal pain?
Treat it as an emergency. Call your GP or go directly to the nearest emergency department. Prompt treatment can prevent permanent damage.
How often will I need follow‑up imaging?
Typically, a scan is done 4-6 weeks after an ERCP or stent placement, then every 6-12 months depending on the underlying cause and symptom stability.
Is an enzyme supplement necessary?
Most patients with a blocked duct develop exocrine insufficiency, meaning their body can’t produce enough digestive enzymes. A prescribed pancreatic enzyme supplement taken with meals helps absorb nutrients and reduces stool issues.










Eunice Suess
October 3, 2025 AT 09:50